Development and Pilot Implementation of a Trauma Registry
Background: Trauma registries (TRs) play an integral role in the assessment of trauma care quality. TRs are still uncommon in developing countries owing to awareness and cost. We present a case study of development and pilot implementation of “Karachi Trauma Registry” (KITR), using existing medical records at a tertiary-care hospital of Karachi, Pakistan to present results of initial data and describe its process of implementation.
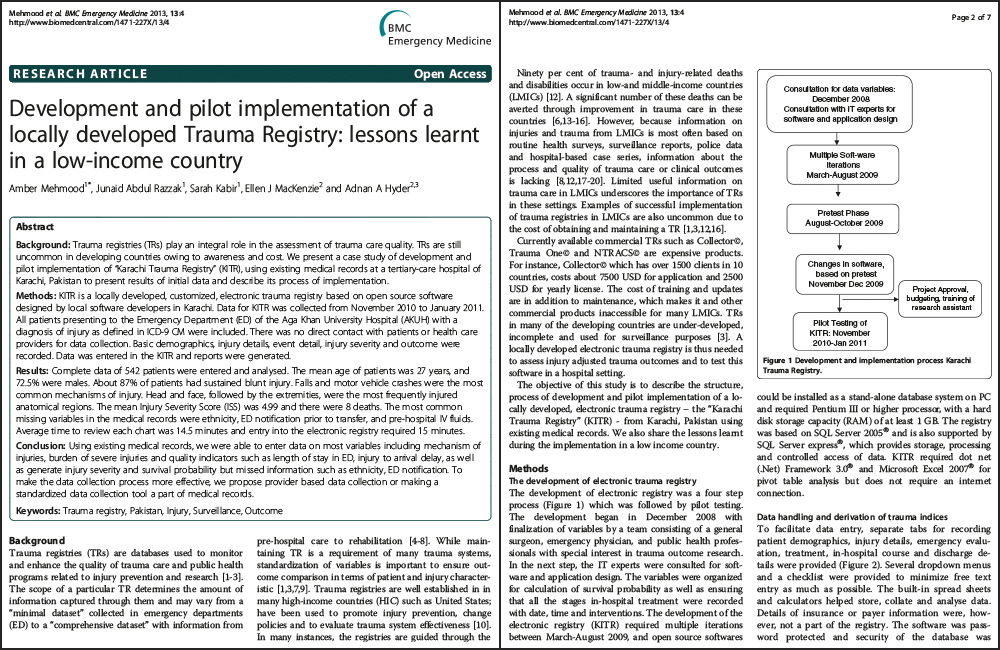
Methods: KITR is a locally developed, customized, electronic trauma registry based on open source software designed by local software developers in Karachi. Data for KITR was collected from November 2010 to January 2011. All patients presenting to the Emergency Department (ED) of the Aga Khan University Hospital (AKUH) with a diagnosis of injury as defined in ICD-9 CM were included. There was no direct contact with patients or health care providers for data collection. Basic demographics, injury details, event detail, injury severity and outcome were recorded. Data was entered in the KITR and reports were generated.
Results: Complete data of 542 patients were entered and analyzed. The mean age of patients was 27 years, and 72.5% were males. About 87% of patients had sustained blunt injury. Falls and motor vehicle crashes were the most common mechanisms of injury. Head and face, followed by the extremities, were the most frequently injured anatomical regions. The mean Injury Severity Score (ISS) was 4.99 and there were 8 deaths. The most common missing variables in the medical records were ethnicity, ED notification prior to transfer, and pre-hospital IV fluids. Average time to review each chart was 14.5 minutes and entry into the electronic registry required 15 minutes.
Conclusion: Using existing medical records, we were able to enter data on most variables including mechanism of injuries, burden of severe injuries and quality indicators such as length of stay in ED, injury to arrival delay, as well as generate injury severity and survival probability but missed information such as ethnicity, ED notification. To make the data collection process more effective, we propose provider based data collection or making a standardized data collection tool a part of medical records.
Specifications
- Last Updated: 2013
- Author(s): Amber Mehmood, Junaid Abdul Razzak, Sarah Kabir, Ellen J MacKenzie and Adnan A Hyder
- Category: Registry Basics
- Tags: 2013, BioMed Central, English
PDF Documents
Please login to access file downloads.